Neuromyelitis Optica: What’s in a Name?
This condition was once called Devic’s syndrome. Our expert, Katy Peters, MD, FAAN, describes the disorder and explains why the name was changed.
This condition was once called Devic’s syndrome. Our expert, Katy Peters, MD, FAAN, describes the disorder and explains why the name was changed.
In “What’s in a Name?” we explore how neurologic disorders get their names and how some of them have changed to reflect new understanding and cultural sensitivities.
We first explored Sydenham chorea, which was once called St. Vitus dance. Here, we talk about neuromyelitis optica, a disorder that was originally named Devic’s syndrome.
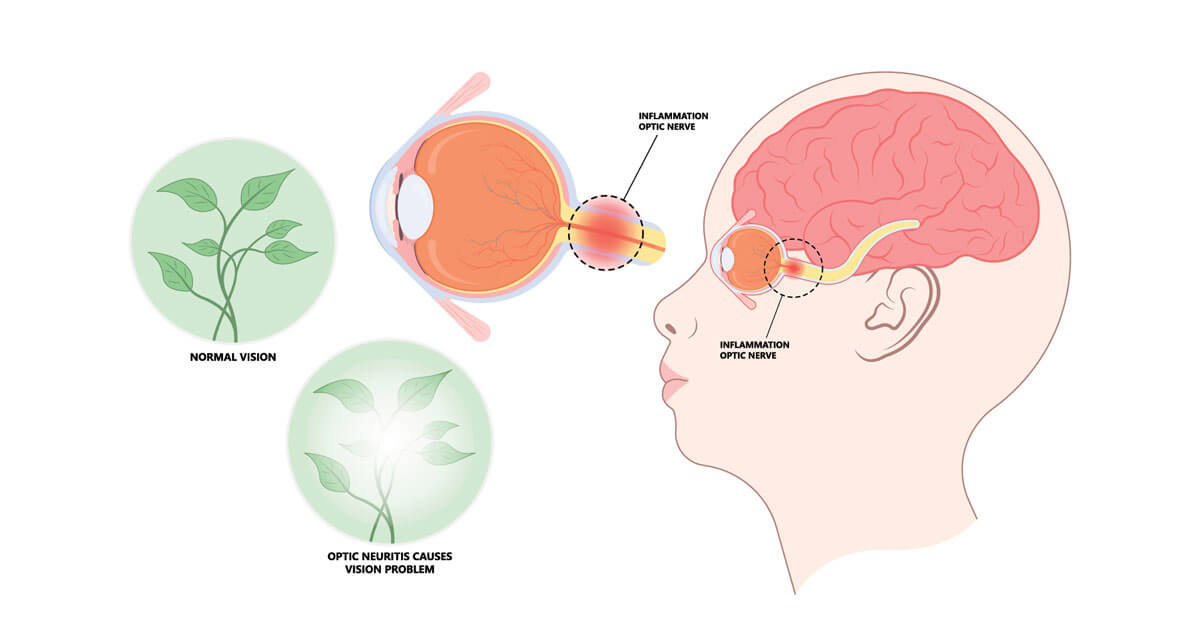
As is the case with many neurologic disorders, the condition that became known as Devic’s syndrome was associated with the physician who was thought to have first identified its unique symptoms. In 1894, Eugene Devic, MD, a French neurologist, observed a case of inflammation in the spinal cord (myelitis) and optic nerve (optic neuritis), which he called “neuro-myelite optique aigue” (neuromyelitis optica in English). Dr. Devic referred to the syndrome by its biological manifestation, but in 1907, the Turkish physician Peppo Acchiote, MD, proposed in a paper that the syndrome be called “maladie de Devic,” or Devic’s syndrome in English.
Dr. Acchiote’s suggestion became accepted parlance among the general public, but neurologists, researchers, and other scientists continued to use the words neuromyelitis optica to describe the disorder. In the intervening 120 years, criteria for diagnosing the syndrome evolved, as did the trend toward referring to it more consistently as neuromyelitis optica, or NMO. Until recently, most neurologists considered NMO a subtype of multiple sclerosis (MS). But in 2004, a team of scientists discovered that people with NMO had an autoantibody in their cerebrospinal fluid that people with MS did not have. Unlike antibodies, which attack foreign invaders like bacteria or viruses, autoantibodies attack healthy tissues. In the case of NMO, the autoantibodies attack a protein called astrocyte water channel protein aquaporin 4 (AQP4), shutting it down and disrupting nerve cell function. Demyelinating diseases like NMO and MS damage the protective coating (myelin sheath) that surrounds nerve fibers in the brain, those leading to the eyes, and those in the spinal cord. When the sheath is damaged, nerve signals slow or stop and cause neurologic problems such as pain, fatigue, and numbness.
NMO, which can occur in children and adults, damages the white matter of the spinal cord and optic nerves. Doctors look for the autoantibody for AQP4 through bloodwork or in cerebrospinal fluid from a lumbar puncture. Symptoms—which typically come and go and are referred to as flare-ups—include vision problems and eye pain, weakness or numbness in the arms and legs, and urinary difficulties. In some cases, patients experience progressive symptoms and may lose their sight.
Doctors order regular MRI scans to look for abnormalities in the optic nerves, brainstem, and spinal cord. For flare-ups, doctors prescribe high doses of corticosteroids or plasmapheresis, a procedure that filters out antibodies to AQP4 from the blood. Immunosuppressants like eculizumab (Soliris), inebilizumab (Uplizna), and satralizumab (Enspryng) can help prevent flare-ups. Side effects include headaches, cold-like symptoms, and fatigue. Because these medications suppress the immune system, patients may experience opportunistic infections.
LISTEN NOW
For more on neuromyelitis optica, listen to the Brain & Life Podcast. MasterChef Christine Ha shares how she has adapted and excelled as a chef despite the challenges that accompany an NMO diagnosis.
Follow and subscribe wherever you get your podcasts!
Apple Podcasts Spotify Libsyn

